
PanNET : Differential



Comments:
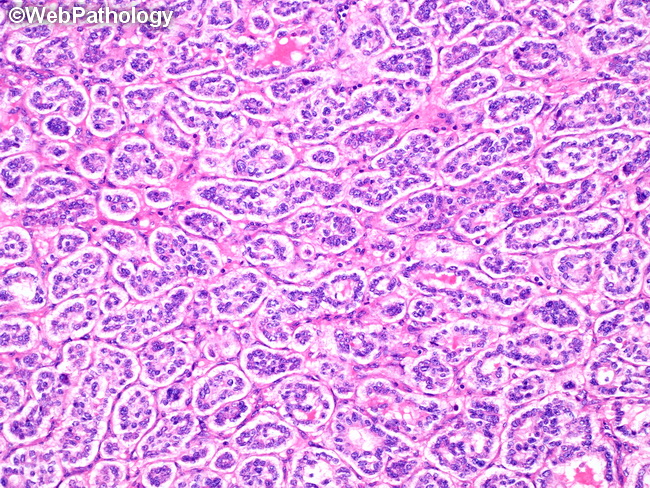
Differential Diagnosis of Pancreatic Neuroendocrine Tumors (PanNETs): PanNETs must be distinguished from pancreatic neuroendocrine carcinoma (PanNEC), acinar cell carcinoma, solid pseudopapillary neoplasm, pancreatoblastoma, and ductal adenocarcinoma of pancreas. Pancreatic Neuroendocrine Carcinoma: Features favoring PanNEC include diffuse infiltrative pattern, necrosis, >20 mitoses/10HPF or 2 sq.mm, desmoplastic stromal response, weak/absent staining with neuroendocrine markers, positive for p53, absent RB1 staining, no loss of DAXX or ATRX staining (i.e. no mutations), and high Ki-67 proliferation index (usually >50%). Acinar Cell Carcinoma: Features include solid and acinar architecture, prominent nucleoli, granular eosinophilic cytoplasm, positive for pancreatic enzymes trypsin/chymotrypsin/lipase; may be focally positive for chromogranin/synaptophysin. Pancreatoblastoma: Features consist of solid and acinar patterns with squamoid nests, immunoreactivity for trypsin/chymotrypsin/lipase, and focal staining with synaptophysin/chromogranin. Solid Pseudopapillary Tumor: SPT has solid, pseudopapillary, and cystic areas; discohesive cells creating pseudopapillary structures; nuclear grooves; eosinophilic hyaline globules; positivity for β-catenin and LEF1 (nuclear), vimentin, CD10, CD56, α1-antitrypsin, keratin (focal) and synaptophysin (focal); negative for chromogranin, trypsin, and chymotrypsin. Ductal Adenocarcinoma: The diagnosis is supported by solid infiltrative pattern, desmoplastic stroma, brisk mitotic activity, mucin production by glands, positivity for CEA, EMA, CK7, and MUC1. About this image: This case of PanNET shows tubular/glandular architecture, minimal atypia, and delicate fibrovascular stroma.