
Cardiac Sarcoidosis : Diagnosis



Comments:
Diagnosis of Cardiac Sarcoidosis (CS):Endomyocardial Biopsy: Due to higher diagnostic yield and comparatively lower procedural risks, extra-cardiac sites such as lung or lymph node are biopsied first. If extra-cardiac biopsies are negative, endomyocardial biopsy may be performed. However, given the focal nature of the disease, endomyocardial biopsy has a low sensitivity and non-caseating granulomas are seen in less than 25% of cases. With the addition of electrophysiologic mapping or imaging modalities (MRI or PET scan) to the biopsy procedure, the positive biopsy rates have reached 50%. In 2014, the first international guidelines for the diagnosis of CS were published by the Heart Rhythm Society in collaboration with a number of other societies. Imaging: Chest x-ray and high-resolution CT are usually abnormal in patients with CS. Ultrasonography is usually abnormal in clinically manifest CS. The findings may include interventricular thinning, left ventricular and/or right ventricular diastolic and systolic dysfunction, wall motion abnormalities, and aneurysms. Cardiovascular magnetic resonance imaging has been found useful in identifying small areas of myocardial damage/fibrosis in clinically silent CS.
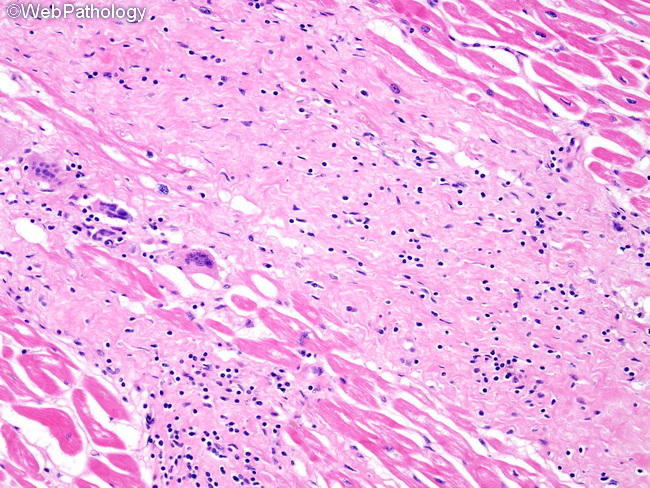
Fluoro-deoxyglucose positron emission tomography (FDG-PET) imaging is capable of differentiating between normal areas and active inflammatory lesions. Inflamed areas have higher metabolic activity and show increased glucose utilization by macrophages and lymphocytes. FDG-PET has been used as a marker of disease activity to guide therapy. Electrocardiogram: Electrocardiogram shows varying degrees of conduction block, ST-T wave changes, and pathological Q waves. Biomarkers: Angiotensin converting enzyme levels are elevated in 60% of patients with sarcoidosis. However, this marker lacks sensitivity and specificity. Other markers that have been found promising include neopterin, soluble IL-2 receptor levels, and highly sensitive Troponin. However, none of them are ready for routine clinical use. Interleukin-6 levels are also usually elevated. The image shows a scar-like area of interstitial fibrosis with multinucleated giant cells and lymphocytic infiltrate.