
Chordoma : Differential Diagnosis



Comments:
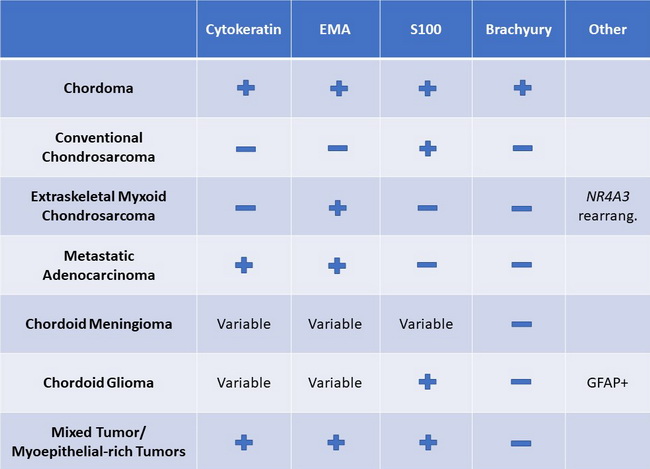
Differential Diagnosis: Chordomas must be differentiated from metastatic carcinomas (especially renal cell carcinoma), chondrosarcoma, meningioma, myoepithelioma/myoepithelial carcinoma, and glioma. This distinction can be especially challenging on small, crushed biopsies since many lesions (especially those arising near the base of skull) can demonstrate similar clinical, CT and MRI findings. An immunohistochemical panel consisting of epithelial markers, S100 protein, brachyury, and GFAP (for skull base lesions) is sufficient in most cases in arriving at the correct diagnosis. See the staining patterns for various entities in the table (Modified from: Wasserman JK, Gravel D & Purgina B. Chordoma of the Head and Neck: A Review. Head and Neck Pathol (2018) 12:261-268. Another differential diagnostic consideration is benign notochordal tumor (BNT) involving the vertebrae or sacrum. It has also been referred to as giant notochordal rest. Features favoring BNT include: no destruction of bone; no soft tissue extension; sclerotic instead of lytic lesion; no extracellular myxoid matrix; bland histologic appearance resembling fat.