
Barrett Esophagus : Treatment



Comments:
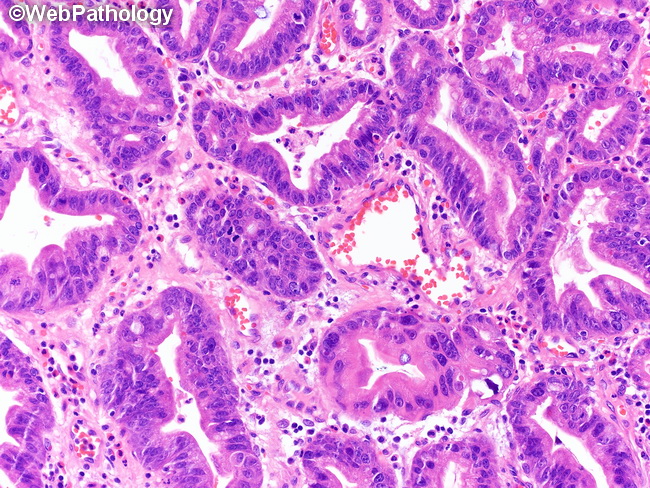
Treatment of Barrett Esophagus (BE): The treatment modalities become more complex once dysplasia is definitively diagnosed. The treatment will differ by institution, but most patients with dysplasia are treated with endoscopic eradication therapy (EET), in the form of ablation, resection, or both. Ablative techniques directly destroy the dysplastic tissue using photochemical energy (photoablation), cold temperatures (cryoablation), or radiofrequency energy (radioablation). Resection techniques are more invasive and involve removal of tissue from the esophagus. These methods include endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD), which involve injection of a submucosal lifting agent to elevate the lesion. Once the lesion is lifted, a diathermic snare or endoscopic knife is used to excise it. The tissue is sent to pathology for evaluation. Esophagectomy for Barrett Esophagus: High-grade dysplasia in BE used to be routinely treated with esophagectomy. It is no longer the preferred method due to associated high morbidity and mortality and the development of less radical approaches; although it remains a valid option in selected cases. It may be considered in patients where dysplastic mucosa cannot be eradicated by endoscopic mucosal resection or in patients with very long segments of Barrett mucosa that have multifocal dysplasia. About this image: High-grade dysplasia in BE (higher magnification of the previous image). The glands are irregular in shape. There is marked variation in nuclear size and shape with piling up of nuclei. There is nuclear hyperchromasia, high N:C ratios, prominent nucleoli and increased mitotic activity as well. When viewed at low magnification, the dysplastic areas stand out due to their basophilia and loss of mucus.