Mar 2016
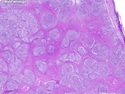
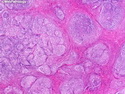
Follicular Lymphoma
Reviewer(s): Dharam M. Ramnani, MD
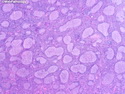
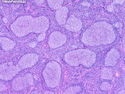
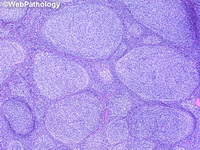
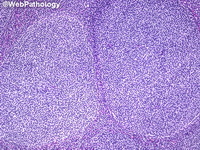
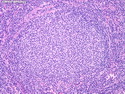
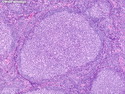
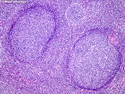
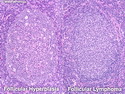
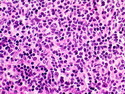
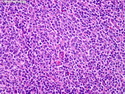
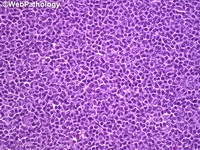
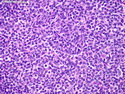
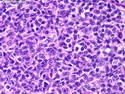
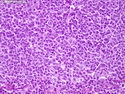
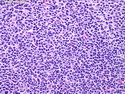
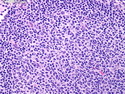
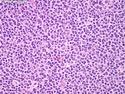
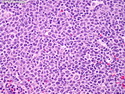
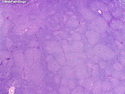
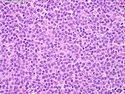
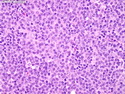
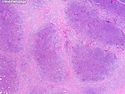
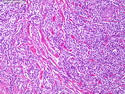
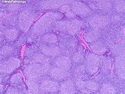
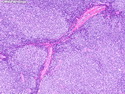
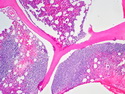
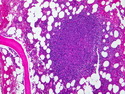
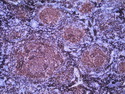
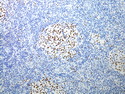
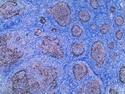
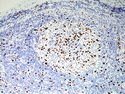
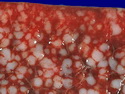
Follicular lymphoma (FL) is a low-grade B-cell neoplasm that makes up 40% of all adult non-Hodgkin lymphoma (NHL) in the US. It is less common in Europe and Asia. It usually occurs in elderly patients. It presents with painless generalized lymphadenopathy. Extranodal sites are less commonly involved. Morphology: Grossly, the involved lymph nodes show nodularity which disappears in advanced cases due to diffuse growth pattern. The neoplastic cells consists of an admixture of small and large lymphoid cells. Centrocytes: The small cells have cleaved or irregular nuclei with infoldings and indentations, coarse chromatin, inconspicuous nucleoli and scant cytoplasm. Centroblasts: The larger cells have round vesicular nuclei, prominent nucleoli, and moderate amount of cytoplasm. Follicular dendritic cells (which are non-neoplastic) are also found within neoplastic follicles. Peripheral blood involvement is seen in about 10% of cases. Bone marrow involvement consists of paratrabecular lymphoid aggregates and is seen in about 40% of cases. Other organs frequently involved are splenic white pulp and portal tracts. Immunophenotype: The neoplastic follicles are composed of monoclonal B-cells which express CD19, CD20, CD22, CD79a and HLA-DR. Surface Ig (IgM type) with light chain restriction and CD10 (60%-70% cases) are also expressed. BCL2 and BCL6 are expressed in vast majority of cases. CD5 and CD43 are negative. Molecular Genetics: About 90% of cases show t(14;18)(q32;q21) translocation which juxtaposes the IGH locus on chromosome 14 with BCL2 gene on chromosome 18 resulting in overexpression of BCL2. BCL2, which is located in the mitochondria, promotes cell survival by opposing apoptosis in the follicles. About 10-15% of FL cases (pediatric FL, primary cutaneous follicle center lymphoma, and grade 3B FL) don't show BCL2 rearrangement.