Jan 2016
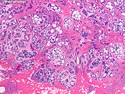
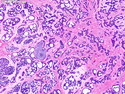
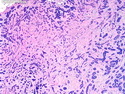
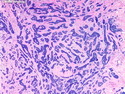
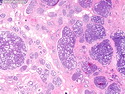
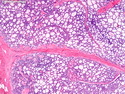
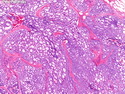
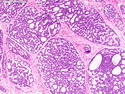
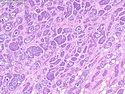
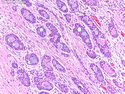
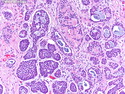
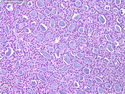
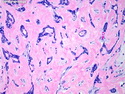
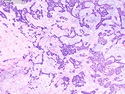
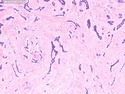
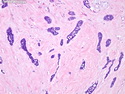
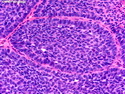
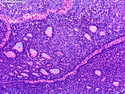
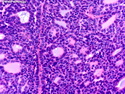
Adenoid Cystic Carcinoma
Reviewer(s): Dharam M. Ramnani, MD
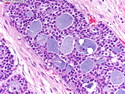
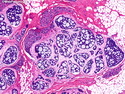
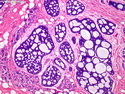
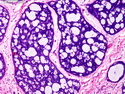
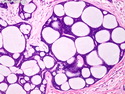
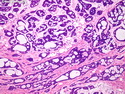
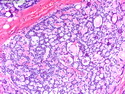
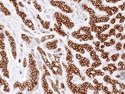
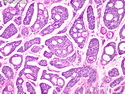
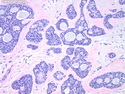
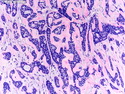
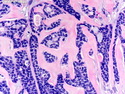
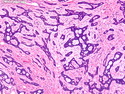
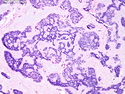
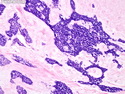
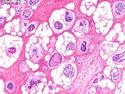
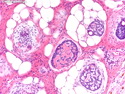
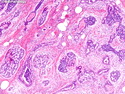
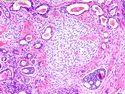
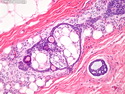
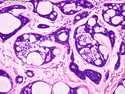
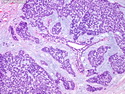
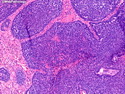
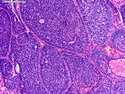
Clinical: Adenoid cystic carcinoma (AdCC) of breast makes up less than 0.1% of all breast cancers. Most patients are post-menopausal and white; the median age at diagnosis is between 50 and 63 years. The usual presentation is with a unifocal, palpable, discrete, firm mass. Morphology: AdCC usually consists of a well-circumscribed central tumor nodule and an infiltrative pattern at the periphery. Gross or microscopic cystic areas are present in about 25% of cases. There is an admixture of proliferating glands (adenoid component) and basement membrane material produced by myoepithelial cells (cylindromatous component). The tumor cells display many growth patterns, including cribriform, tubular, trabecular, solid, and basaloid. Uncommon features include sebaceous metaplasia (14% of cases), squamous differentiation, adipose differentiation, metaplastic spindle cell stroma, and syringomatous areas. A small percentage of cases show perineural invasion and lymphovascular invasion. Immunohistochemistry: AdCC are negative for hormone receptors ( ER, PR, AR) and Her2. Most cases show strong positivity for CD117/c-kit (membranous) and p63 (nuclear). Overexpression of MYB protooncogene can be detected immunohistochemically in many cases. Molecular Genetics: AdCC of salivary glands, breast and other locations carry a specific chromosomal translocation t(6;9)(q22-23;p23-24) resulting in MYB-NFIB gene fusion. This alteration can be detected by FISH and RT-PCR. MYB overexpression has been detected immunohistochemically in tumors with and without MYB-NFIB fusion. Differential diagnosis:The differential diagnosis of AdCC includes collagenous spherulosis (non-palpable, CD117 negative), invasive cribribriform carcinoma and cribriform DCIS (monophasic with no myoepithelial component, no matrix deposits), solid papillary DCIS, high-grade carcinoma arising in microglandular adenosis (no myoepithelial cells, p63 neg.), and benign adnexal lesions such as syringomatous adenoma and cylindroma. Treatment & Prognosis: The preferred treatment is breast-sparing conservative surgery. Mastectomy is reserved for large tumors. Adjuvant radiotherapy appears to reduce the rate of local recurrence. Adjuvant chemotherapy is rarely used. Axillary lymph node metastases are uncommon. Rare patients can develop pulmonary metastases several years after initial treatment. However, the overall prognosis is good with a low risk of systemic metastasis and death from AdCC. Ref: Rosen's Breast Pathology, 4th Ed., 2014; Rosai's Surgical Pathology, 10th Ed., 2011.